

Work and health: international comparisons with the UK
A report for the Commission for Healthier Working Lives
Executive Summary
Economic inactivity due to ill health is a persistent challenge facing many countries. However, there are substantial differences in the extent of the challenge, which segments of the working-age population fare better or worse, and in the mechanics and scope of government work and health policies.
This report – one of a series informing the Commission for Healthier Working Lives – investigates how the UK compares with 14 other European countries in the employment of workers with long-term ill health or disabilities. It also reviews relevant policy interventions and practices from around the world to draw potential lessons for the UK.
Work-health differences between the UK and European nations
Our analysis uses nationally representative data from 15 European countries – the ‘EU15’, comprising the EU members from 1995 to 2004, a period when the UK was part of the European Union. We show that, relative to its European peers, the UK underperforms in the employment outcomes of people with long-term ill health. While workers with health limitations often face employment challenges, these challenges appear especially pronounced in the UK. In most areas, though not all, the UK is among the worst performers in the EU15. We see this across age groups but there are especially concerning signs for younger UK adults.
Our analysis of the employment prospects of workers with ill health includes changes from pre- to post-pandemic (2018 to 2022) and uses multivariate analysis to control for a range of other factors, such as sex, age, marital status, and education. This method is important for international comparisons, as it accounts for differences in population and labour markets. By enabling like-for-like comparisons, the analysis isolates the ‘true’ country differences in ill health and employment. While volatility in prevalence measures over time may affect observed changes, the patterns identified point to a growing challenge for the UK:
- Between 2018 and 2022 there was a reduction in the employment rate of people with health limitations in most European countries. The UK ‘employment gap’ between those with and without health limitations is shown by available data to be among the highest in the EU15.
- The rise in worklessness among young UK adults with health limitations is especially pronounced. People aged 16-24 with health limitations were more than twice as likely to be out of work in 2022 than they had been pre-pandemic.
- For older workers with health limitations, employment chances are declining in the UK, but improving elsewhere. Between 2018 and 2022, the likelihood of being out of work due to ill health decreased for people aged 55–64 in most EU15 countries but increased in the UK. While the UK is still only slightly worse than average in this regard, it appears to be headed in the wrong direction.
It is important to note that cross-country comparisons of work and health outcomes are subject to limitations in data comparability, which are not explored in detail here.[1] Despite this, the findings highlight ongoing concerns for the UK, which are broadly consistent with previous evidence. More detailed research is needed to better understand the limitations of cross-country comparisons and how such comparisons can better guide policy decisions.
Potential policy lessons from overseas
We follow our analysis of international data with a rapid review of work and health policies and practices from a range of countries, considering potential lessons for the UK. A separate paper in this series takes a closer look at current UK policies on employment and health and the most promising areas for improvements.
In this paper, we illustrate how approaches to workplace health vary across countries. At the broadest level, there are clear differences in how integrated policies on workforce health are, and how tightly they define responsibilities for different actors, in particular employers. The UK is among the countries with less integrated approaches. The risk with less integrated approaches is that policy is less proactive and coherent, with the result that workplace health support can be harder to access. Early intervention to support people at risk of leaving work due to health problems is key to improving outcomes.
In our review of specific policies and interventions, we group measures into three areas: healthy work, staying in work, and getting into work.
Measures to ensure healthy work
Interventions include:
- Working time legislation. Many countries, including the UK, have implemented limits on the number of hours people can work. In some countries, this now includes an employee ‘right to disconnect’. Reductions in working hours with retained salary has been shown to be effective at improving some indicators of wellbeing, but evidence on the effectiveness of legislation is mixed.
- Employer incentives to improve practice. Interventions such as grants and subsidies for employers to adopt good practice can have a positive impact, but can also be contingent, for example on inclusive decision making processes.
- Industry-focused initiatives. Programmes targeted at specific industries, for example encouraging employers to share good practice, can bring small to moderate improvements.
Measures to help people with ill health and disabilities stay in work
- Occupational Health (OH) services. OH delivery models vary by country in terms of who delivers them (for example, in-house or external physicians) and whether employers are mandated to provide them. Countries with a more integrated policy framework around workforce health tend to have higher OH coverage.
- Sickness pay. In several European countries, statutory sick is linked to an individual’s wages, unlike the UK’s fixed-rate system. These models tend to provide a higher rate of income replacement than in the UK.
- Rehabilitation and workplace adjustments. Unlike the UK, various European countries provide active support to help workers transition back into employment after sickness absence.
Measures to help people move out of economic inactivity and get into work
- Anti-discrimination laws. There is little evidence that these kinds of laws improve the likelihood of disabled people being in work.
- Mandated employment quotas. Some countries apply even stronger legislation, requiring employers to meet quotas for hiring disabled workers. Evidence here is mixed, pointing to some positive impact, but also unintended consequences such as increased stigma.
- Workplace adjustments. Practice varies across European countries, from providing expert advice or adaptation grants, to the extent of external support and how much cost employers must cover. Successful systems focus on aspects of job quality, such as flexibility in how a job is performed, and expand access to adjustments to lower-paid workers.
- Employer incentives for hiring disabled workers. Employment subsidies are present in some European countries, but evidence on their effectiveness in supporting entry into the open labour market is mixed.
Conclusions
There is good evidence that the UK can improve the employment prospects of people with ill health and disabilities, enabling more people to benefit from employment and actively contribute to the economy. Improvements seen in many European peers suggests that this is possible. Change needs to happen across the board, but younger workers should be a particular priority, given recent trends and the long-term consequences of being out of the labour market early in a person’s career.
Policy interventions addressing work and health vary in delivery mechanism, and scope of population targeted, so there are a range of options at our disposal. The UK government should carefully consider what changes are most likely to lead to sustained improvements, drawing on examples illustrated in this report.
However, it is arguably very important to ensure long-term consistency and develop policy that works in consort to create a cohesive system. So, balanced against making necessary changes, policy makers should aim to stick to a coherent, long-term plan.
Another systemic consideration is how the key actors – government, employers, employee representatives and private sector service providers – work together. This concerns the basic industrial relations framework of a country and the capacity of different actors to take a lead. At a more detailed level, there are lessons to be learned from industry-wide initiatives.
Finally, the effectiveness of policies and interventions in practice will inevitably be affected by the level of awareness and the willingness of employers and other actors to engage with them. Attitudes towards ill health and work will be influential here. They will also be instrumental in de-stigmatising physical and mental ill health in the workplace, enabling comprehensive OH services that are relevant to job demands and not ‘over-medicalised’ – for example, focusing on health promotion as well as illness – and in reducing under-reporting of ill health.
This report highlights a wealth of international examples of policy interventions that differ in strength, mechanism and scope. Careful consideration should now be given to what changes are most likely to lead to sustained improvements in the UK, enabling more people with long-term ill health or disabilities to benefit from employment and actively contribute to the economy.
1. Introduction
Background
Economic inactivity due to ill health is a persistent challenge facing many countries. A 2010 report by the Organisation for Economic Co-Operation and Development (OECD) noted that:
‘Too many workers leave the labour market permanently due to health problems or disability, and too few people with reduced work capacity manage to remain in employment. This is a social and economic tragedy that is common to virtually all OECD countries.’[2]
Nonetheless, there is significant variation in how different countries approach these issues and, more specifically, in how well they have recovered from the COVID-19 pandemic. As we shall see, the United Kingdom (UK) has particularly struggled with regards the latter.
This report is part of a series supporting the Commission for Healthier Working Lives. The first section addresses gaps in analysis by comparing work and health outcomes in the UK with those of European peers, focusing on trends across different population groups, particularly by age. The second section examines approaches to workforce health adopted in other European countries, exploring what has been effective and why, to inform UK policies and interventions. A separate paper in this series provides a more detailed analysis of the current UK policy landscape.
Research questions and approach
This report seeks to address three key questions:
- What differences exist between the UK and other developed economies in the prevalence of poor health among people of working age and the likelihood of those with health conditions being in work?
- What does research evidence tell us about approaches that have worked overseas?
- What are the potential implications for UK public policy and workplace practices?
We take a mixed methods approach involving:
- Quantitative analysis. Focusing on European countries, where data is most accessible and comparable, particularly the EU15 (the 15 European Union countries from 1995 to 2004, including the UK). We use data from EU statistics on income and living conditions (EU-SILC)[3] for 2018 and 2022 alongside 2022 UK data from Understanding Society: The UK Household Longitudinal Study (UKHLS).[4] These datasets are broadly consistent, although there are some limitations to the data comparability across countries.[5] We conduct descriptive and multivariate analyses exploring country differences in the prevalence of ill health and the employment of people with health conditions. For more details on the data and our methods, see Appendix 1.
- Desk-based research. A brief review of approaches taken in other countries, particularly drawing on existing evidence syntheses. The review is not systematic but aims to provide a general sense of international differences.
- Roundtable discussion. Findings were discussed with experts in European workplace health and related policy.
Structure of the report
Section 2 sets out findings from the new analysis of EU-SILC and Understanding Society data.
Section 3 reviews different national approaches, exploring what may work or what could improve the effectiveness of workplace health policies.
Section 4 draws together conclusions and implications from the previous sections, discussing factors that may explain cross-country differences.
2. Work-health differences between the UK and European nations
Key findingsMany workers with health limitations face employment challenges, but these challenges appear more pronounced in the UK than across many comparable European countries. Among the ‘EU15’ European countries examined, the UK ranks among the worst performers in most areas. Key findings include: · The UK has one of the highest reported rates of health limitations among those aged 16–64 in the EU15. · The UK’s employment gap between those with and without health limitations is among the widest in the EU15. · Between 2018 and 2022, there was a general decline in employment rates for people with health limitations across the EU15. · In the UK, the likelihood of being out of work for those aged 16–24 with health limitations more than doubled between 2018 and 2022. · While the likelihood of being out of work for those aged 55–64 decreased for most EU15 countries over this period, it increased for the UK. |
Background
The UK faces a significant socio-economic challenge in the post-COVID landscape, with a marked rise in economic inactivity[6] and receipt of incapacity benefits. Total jobs and employment levels in the UK might be higher than those reported in recent official statistics,[7] suggesting that UK’s apparent divergence from other OECD and EU countries may be less significant than initially thought. Even so, the employment consequences of ill health and disability remain a critical issue.[8]
A recent OECD report examined employment opportunities for people with disabilities across countries, concluding that those with disabilities and/or health limitations continue to be disproportionately excluded from the labour market.[9] It argued that:
‘… the implementation of actual change has fallen short of what is needed to achieve substantially better employment outcomes and greater labour market inclusion of people with disability’ – OECD, 2022
The report also highlighted that, at the time of writing, the impact of the COVID-19 pandemic was still unfolding. Some OECD countries, including the UK and Denmark, had seen notable improvements in the employment rate of people with health limitations and/or disabilities prior to the pandemic. In contrast, several other OECD countries, including Germany, Greece, Ireland and Italy, had seen a reduction in employment rates for this group.
In this section, we present new data analysis that builds on these findings.
Data analysis
The 2022 OECD report used EU-SILC data covering the pre-pandemic period. The analysis in this report builds upon the OECD findings in two ways.
First, we extend the analysis to the post-pandemic period, comparing data from 2018 with data from 2022. We do this to give a more up-to-date picture of the prevalence of health limitations and the employment rates of those with and without such limitations. The volatile period of the COVID-19 pandemic between 2018 and 2022 saw rapid changes in health and employment support policies. The different paths followed by European countries in managing the crisis and supporting the labour market makes this an interesting, though challenging, period to examine.
Second, we conduct a ‘marginal effects’ analysis. To isolate the ‘value-added’ effect of each country, we use this technique to estimate how being resident in a specific country influences work and health outcomes when accounting for other factors. This approach provides valuable information about the country effects related to the prevalence of health limitations and its association to employment rates. The marginal effects analysis examines these outcomes across different age groups and genders.
See Appendix 1 for more information on the data and analysis methods.
Employment of those with ill health
General levels of ill health vary greatly
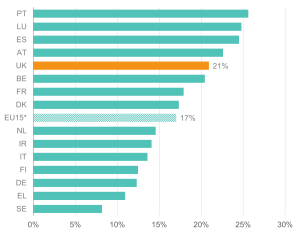
The data reveal substantial variation in the reported prevalence of health limitations across European countries. These differences are likely to reflect both variations in underlying health conditions and differences in reporting or definitions. Rates are comparatively low in Sweden, Greece, Denmark, and Finland but notably higher in Portugal, Luxembourg, and Spain. At 21% of 16-64-year-olds reporting health limitations, the UK is above the EU15* average (Figure 1).[10] The estimated prevalence of health limitations in the UK for 2022 closely resembles the OECD estimate of the prevalence of disability in the UK in 2018.[11]
Figure 1: The reported prevalence of health limitations is higher in the UK than in many European countries
Proportion (%) of people aged 16-64 reporting that they suffer from a chronic (long-standing) illness or condition; EU15 countries, 2022
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Employment participation of people with health limitations
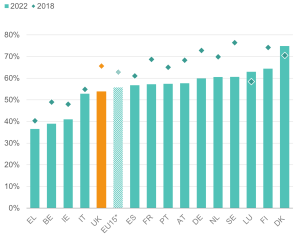
Employment rates for people reporting health limitations seem to have decreased across many European countries between 2018 and 2022. Among the 15 countries examined, only Denmark and Luxembourg registered a higher rate of employment for those aged 16-64 with health limitations during this period (see Figure 2). The UK is among the countries where the employment rate for people with health limitations has deteriorated the most since 2018, despite showing strong improvements prior to the pandemic.[12]
Figure 2: Employment rates of people with health limitations fell across many European countries between 2018 and 2022
Employment rate (% aged 16-64) for people reporting that their health is limited or severely limited in EU15 countries, 2018 and 2022
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
This deterioration aligns with previous research highlighting a disability disadvantage in hiring practices across some European countries, including the UK.[13]
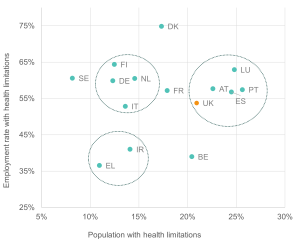
We also plot the association between the reported prevalence of health limitations in the population and the employment rate for people with health limitations across 15 European countries. Figure 3 shows some noticeable clustering of countries across these dimensions, with the UK more aligned with countries like Austria and Portugal.
Figure 3: The UK’s performance places it among the countries with more health limitations and slightly below average employment outcomes
Employment rates of those with health limitations vs. proportion of people with health limitations: people aged 16-64, selected (EU15) countries, 2022
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
The ill health ‘employment gap’
The UK has historically been a relatively high employment economy, although there are indications it has fallen back compared to other European countries since the COVID-19 pandemic. While the OECD reported improvements in the employment of people with disabilities between 2008 and 2018, recent data suggests this trend has reversed.
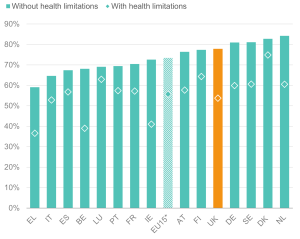
Figure 4 shows that the UK retains a high employment rate for people without health limitations, in line with other northern and Scandinavian countries. However, the gap between the employment rates for people with and without health limitations in the UK is among the largest observed (Figures 4 and 5). Among the 15 countries examined, only Ireland and Belgium show a larger gap. In contrast, the smallest employment gaps are observed in Luxemburg, followed by Denmark, Spain, Italy and Portugal.
Figure 4: While the UK has a comparatively high employment rate for people without health limitations, it has a lower rate for those with health limitations
Employment rate (% aged 16-64) for people with and without health limitations in EU15 countries, 2022
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure 5: The UK’s ill health ‘employment gap’ is one of the widest among the EU15* countries
Percentage point gaps in employment rates between people with and without health limitations in EU15 countries, aged 16-64, 2022
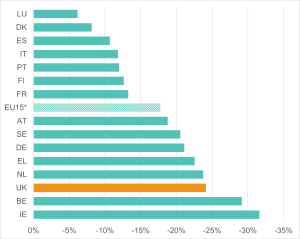
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Note: Employment rate gaps are calculated relative to those without limitations.
Figure 6 sheds further light on the relationship between the prevalence of health limitations and employment outcomes. It plots the employment gaps between those with and without health limitations against the share of 16-64-year-olds with health limitations; in contrast to Figure 3, this indicates how great a difference health limitations make.
The UK’s position in the lower right of the figure reflects a comparatively high share of people reporting health limitations alongside a substantial health employment gap. Countries in the top right, such as Luxemburg, Spain, and Portugal, also have high shares of people with health limitations but with narrower employment gaps. Meanwhile, countries like Germany, Greece and Sweden appear to have some of the lowest shares of people reporting health limitations but display employment gaps similar to those seen in countries with higher shares of people with health limitations.
Figure 6: The UK and Belgium are countries with similar prevalence of health limitations and the ill-health employment gap
Employment rate gap (percentage points) vs. proportion of people with health limitations; people aged 16-64 in EU15 countries, 2022
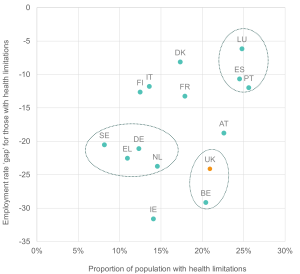
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
OECD analysis shows that accounting for the prevalence of health limitations can partly reduce cross-country differences in employment gaps. However, this also risks blurring the specific impact of health conditions on employment outcomes.[14]
The geographic variation across European countries suggests that north-south or east-west distinctions are not a reliable way to explain the phenomena examined in this study. The variety of outcomes observed may stem from a range of factors, including economic conditions, cultural norms, social security design, population dynamics, policy and political choices, or a combination of these and other factors.
The UK’s deteriorating record on people working with ill health
To examine the specific country effect on the employment of people with health limitations in more detail, we now turn to marginal effects analysis (see Appendix 1 for methods). This section explores the likelihood of individuals with health limitations being out of work in selected European (EU15) countries, with a focus on the UK’s position, between 2018 and 2022. It highlights key patterns by age groups, offering insights into the impact of broader labour market dynamic shifts across time and on different ages.
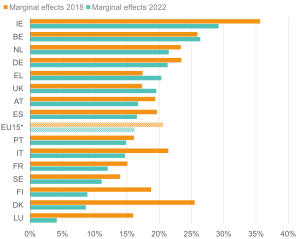
Figure 7: Workers with health limitations face a higher likelihood of being out of work in the UK than in most EU comparators
Likelihood (margins) of being out of work for 16–64-year-olds with health limitations; EU15 countries, 2018 and 2022
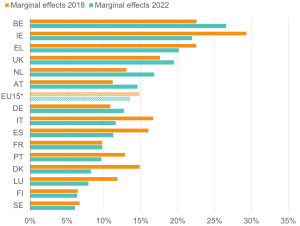
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure 7 shows the marginal probabilities of people with health limitations being out of work across European countries – that is, the additional likelihood of someone with a health limitation being out of work, compared to someone with a similar set of characteristics without a health limitation. This analysis adds to the discussion on employment rates of people with health limitations across EU15 nations by highlighting country differences affecting likelihood of being out of work. Country differences can be attributed to various socio-economic, political, and cultural factors captured in the model. We are thus able to describe the ‘value-added’ effect of each country before and after the COVID-19 pandemic.
Our analysis confirms that the UK performs worse than many other European countries in employment outcomes of those with ill health, although some countries, like Belgium and Ireland, perform worse overall (Figure 7).
Breaking this analysis down by age, the UK performs comparatively poorly for younger adults with health limitations, but somewhat better for older workers. The employment outcomes for people with health limitations have worsened across age groups in the UK, but especially for younger age groups (aged 16-24; see Figure 8).
Figure 8: The UK performs relatively poorly on the employment outcomes for young adults with ill health
Likelihood (margins) of being out of work for 16–24-year-olds with health limitations; EU15 countries, 2018 and 2022
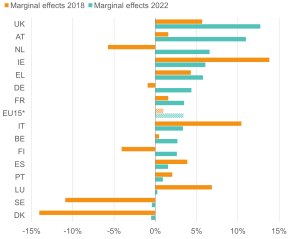
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society Note: The negative margins suggest that the value added to the probability of employment in those countries is higher for people with health limitations.
Having a health limitation made young people 6% more likely to be out of work in 2018; in 2022 this had worsened such that they were 13% more likely to be out of work. The situation for the young adults seems particularly troubling, with an evident increase in the worklessness of young adults with ill health during the pandemic, even in some Nordic countries that traditionally offer increased support for disadvantaged groups.
However, even with this increase of more than double, the likelihood of being out of work for younger workers falls short of that for older workers aged 55-64, which in 2022 was 20% (Figure 9).
To some extent, these differences may reflect the greater severity of health limitations which appear with age. However, an alternative explanation is that there is an imbalance in how labour market interventions are targeted at different age groups. Additionally, health limitations potentially affect the employment choices of different age groups differently, being a greater influence for those closer to retirement age.
Figure 9: The UK supported older workers with ill health relatively well in 2018, but its relative position worsened by 2022 as other countries improved
Likelihood (margins) of being out of work for 55–64-year-olds with health limitations; EU15 countries, 2018 and 2022
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society Note: For figures on other age groups refer to Appendix 1: Marginal effects regression analysis.
3. Policy lessons from overseas
| Key findings
This review examines work and health policies in a range of national settings, including ‘Type A’ countries that take more proactive and coherent approaches and ‘Type B’ countries that have looser legislative frameworks and often rely more on markets-driven approaches. Effective or promising policies include: · Measures to ensure healthy work, such as working time regulation, incentives for employers and industry-focused initiatives. · Measures to help people with ill health and disabilities stay in work, including occupational health services, statutory sickness pay, and support with rehabilitation and workplace adjustments. · Measures to help people move out of economic inactivity and into work, including anti-discrimination legislation, quotas for employing disabled workers, workplace adjustments and employer incentives for employing disabled workers. |
In Section 2, we presented evidence that the UK has clear room for improving work outcomes for people with ill health or disabilities compared to European peers. The current section reviews policies and interventions from other countries that could help explain why some achieve better outcomes. Drawing lessons from other countries is not straightforward, as policies that succeed in one context may not translate effectively to another. We therefore make comparisons with some caution seeking to highlight the features of mechanisms and approaches that work to inform the best course of action for the UK.
We start by summarising different broad structures for work and health policies before reviewing examples of policies and interventions across three key areas:
- Healthy work: ensuring work is protective and supportive of good health.
- Staying in work: support to keep people with health issues attached to the labour market.
- Getting into work: supporting engagement or re-engagement for those outside the labour market because of health issues.
Structure of workplace regulation and labour standards
A recent DWP report described two broad types of approaches to regulation on occupational or workplace health, summarised in Table 1.[15]
Table 1: High-level policy contexts for ill health and employment
| Type A | Type B |
| A single legislative framework and enforcement ‘with focus on an integrated, multi-disciplinary service, stipulating rights and roles of employers and employees’. These countries often have a strong tradition of social partnership and collective bargaining, which shapes their approach to workplace health. Examples include France, the Netherlands, Poland, Finland, Japan, Italy and Germany. | Legislation is more dispersed across social security, health and safety, and labour laws’, typically with less regulation than in Type A countries. These countries, often English-speaking, rely more on individual responsibility and market-driven policies. Examples include the UK, Canada, Australia, the USA and the Republic of Ireland. |
Type A approaches are generally more proactive and coordinated, resulting in broader coverage of occupational health and related support. These systems often impose greater obligations on employers and integrate preventive and rehabilitative measures into legislation. Specific examples of how these approaches are implemented are explored below.
The DWP report describes Type B legislative frameworks as more ‘open to interpretation’ with the provision of OH services being driven by employers. This can lead to bigger gaps in access, particularly for smaller employers or workers on precarious contracts. Type B countries also rely more heavily on general practitioners (GPs) to provide advice and support to workers with ill health.
Some Type B countries integrate OH services within their general healthcare systems (e.g. Canada, Australia, and the USA). However, access to these services is frequently associated with private insurance (either self-funded or offered as an employer benefit) and eligibility can depend on specific conditions.
Nonetheless, despite these gaps, Type B approaches can still demonstrate proactive elements.
Healthy work: Ensuring work is protective and supportive of good health
Working time legislation
There is a clear link between excessive working hours and health.[16] Working time legislation is commonly used as a way of limiting the total number of hours worked, though regulatory approaches differ. Some countries regulate absolute maximum working hours, while others focus on establishing maximum normal working hours, aiming to treat overtime as an exception.[17]
- In response to a long-hours working culture in Korea, where 18% of workers reported working more than 55 hours per week, its government reduced overtime limits to bring the maximum statutory working hours down from 68 to 52 hours per week.[18]
- Like other countries in the EU, the UK applies the Working Time Directive, which limits the average working time for employers to 48 hours per week, including overtime. Implementation varies across countries. In the UK a unique opt-out provision was incorporated: this allows employees to voluntarily exceed this limit if they consent in writing.
- In Denmark, the Working Time Directive is implemented alongside collective agreements that provide a framework for additional flexibility. These agreements aim to balance employee needs and employer demands,[19] requiring employers to consult with workers through unions or work councils, although final decisions on working hours rest with the employer.
Building on this, a number of countries have also established the ‘right to disconnect’, which legislates for employees to be able to disengage from work-related communications outside work hours.[20] For example:
- France established a law in 2016, following earlier efforts to encourage businesses to avoid intruding on employees’ private lives by specifying when devices should be switched off. Nonetheless, this is seen to still be an opt-in policy in practice.[21]
Other European countries that have implemented similar measures include Belgium, Italy, Germany, Luxembourg and Slovakia. Elsewhere, Australia and Canada recently introduced comparable right to disconnect legislation.
Reduced working hours (with retained salary) have been found to result in a range of health benefits, including better sleep, reduced stress and improved quality of working life.[22] However, employee input is important. Flexible working practices that are driven by organisational needs alone can have negative effects of worker health.[23] Evidence from the UK suggests although the introduction of the Working Time Directive coincided with a decline in the share of workers working excessive hours, the impact of the legislation was unclear.[24]
Workplace representatives and tripartite agreements
Employee voice – whether direct or indirect via representation – is an important mechanism for maintaining workplace health standards and tailoring interventions.[25] There are many examples of policies that set requirements on representation and engagement to uphold healthy workplaces. For example:
- The Japanese government mandate that workplaces with 10 to 49 employees appoint ‘health promoters’ and those with over 50 employees appoint ‘health officers’ to implement OH activities in the workplace.[26] Since 2015, employers with more than 50 employees are also required to conduct annual stress checks with their employees.[27] The stress check is designed to provide data to individuals and employers to support change.
- Under Dutch law, the Working Conditions Act (1994) requires employers with more than 50 employees must form work councils to approve company polices on occupational health and safety policy and absenteeism.[28] Employers are also required to offer employees a regular health examination to identify any health problems arising from their work.[29]
- In Germany, work councils have the power of veto over working time agreements. These co-determination rights mean that employers are required to engage with unions and work councils on working time issues (e.g. working hours and scheduling rules).[30]
The strength of employee representation can significantly shape occupational health outcomes. Stronger representation, as seen in Germany, is associated with healthier outcomes compared to countries with less employee control. Strengthening worker representation could be particularly beneficial in sectors where workers have declining informal bargaining powers[31] or countries with less robust legislative protections (e.g. Type B systems).
Incentives and subsidies
Creating incentives – financial or otherwise – for employers to make improvements to workplace health is one obvious option for government policy.[32] Countries vary in the forms such incentives take, as well as the extent to which they are leveraged.
- In the Netherlands, it has been observed in general terms that reforms in the 1990s and 2000s transformed occupational health services into a more competitive market in which private insurance companies became key players and employers were given financial incentives to invest in the ill health prevention and the reintegration of sick employees.[33]
- More specifically, in Australia, grants are available at a regional level for employers to promote health and wellbeing in the workplace.[34] These focus on mental health and musculoskeletal disorders, as well as return-to-work programmes.
- The Japanese government encourages employers to adopt health and wellbeing initiatives through a national programme of certification and awards. In 2014, the Ministry of Economy, Trade and Industry launched the Health and Productivity Management Programme.[35] The programme provides both certification and awards for employers who take measures to promote health and wellbeing in the workplace, applying a lighter-touch assessment process for SMEs. By 2021, around 13% of Japanese employees were thought to be working in recognised organisations. The data gathered as part of the certification process is used by the government to assess the impact on health and labour market outcomes and reported to organisations to allow them to identify areas for development.
Evidence suggests that such government funding for workplace health interventions can bring about positive change for worker health.[36] However, in the case of the Netherlands, evidence suggests that incentives alone were insufficient to improve outcomes. Benefits were only seen after infrastructure was introduced to allow employers, employees and occupational health professionals to be involved in decisions on how the funds were designed and administered.[37]
Industry initiatives
There are important differences in exposure to health risks by industry.[38] Recognising this, some governments work with partner organisations to support healthy workplaces. The examples below highlight scope for policy initiatives that facilitate knowledge sharing between employers, particularly when focused on specific industries. The UK could draw lessons from how these initiatives have been developed and implemented.
- In Germany, the national government worked with the 16 states and a group of accident insurance organisations to produce a plan for the safe handling of carcinogens and prevent psychological strain and musculoskeletal workload.[39]
- In Poland, the Ministry of Health worked with occupational health centres of expertise to promote healthy lifestyles within workplaces. This included delivering national projects and producing materials, tools and campaigns tailored for employers, employees and occupational health professionals.[40]
- In the Netherlands, the Ministry of Social Affairs and Employment developed a program for knowledge sharing between employers on occupational safety.[41] This bottom-up, sectoral approach focused on practical knowledge of causes of accidents and effective OH solutions, based on initiatives by individual companies or groups of companies. Through employer networks, it aimed to leverage the benefits of learning from peers who work in similar environments.
A systematic review of workplace health interventions in male-dominated industries – such as agriculture, construction and manufacturing – found that they can have small to moderate impacts, depending on delivery method and industry.[42] For example, face-to-face delivery can be less impactful than web-based, which can be more cost-effective and scalable, and more suited to remote and shift workers. This review also found that interventions focused on musculoskeletal disorders showed positive outcomes, whereas studies focusing on lifestyle, mental health and nutrition showed negative or no outcomes.
There is also evidence that trade or industry associations, especially those with larger companies, are well-positioned to promote workplace health initiatives. This can occur through industry-relevant information and guidance and business cases that illustrate the benefits of workplace health interventions. One study observed this potential in the mining, transport, agriculture, manufacturing, farming, hospitality, and construction industries.[43] However, it also noted that confusion could arise about what are government-mandated policies and what are non-mandated initiatives.
Staying in work: Support to keep people attached to the labour market
There is good evidence that there are benefits from structured approaches to returns to work from sickness absence. We can thus expect benefits from policy measures that promote such approaches.
Occupational health services
OH professionals commonly feature in national approaches to supporting health at work, including in the UK. The level of funding and support from government varies considerably but employers consistently play a central role in both funding and administering OH services.[44] There are differing models not only between countries but also within them (with mixed approaches to OH provision being common). These can include in-house OH services, bespoke private provision, group models in which employers make a yearly financial contribution per employee, social security models, and community-based health centres.
- In Finland, the Act on Occupational Health Services imposes a duty on employers to fund preventive health care for employees, provided by a relevant specialist (e.g. a nurse or occupational psychologist).
- In France, large organisations have long been required to have occupational health nurses.[45] These tend to be either in-house or group-level provision. OH is funded directly by employers and, in a Bismarck model, by regional authorities via employer contributions.
- In the Netherlands, employers are legally mandated to provide OH under the Working Conditions Act (1994). During sickness absence, a gatekeeper protocol mandates tasks for employers, employees and OH physicians to support a return to work. This includes referring employees to OH for an assessment and drafting an action plan to provide suitable work.
- Extending an aspect of Dutch policy, Japan also has a legal mandate for organisations of more than 50 employees to appoint a dedicated OH physician. For smaller organisations a part-time occupational physician must be contracted. There is also an emphasis on legislation on primary prevention, and all workplaces are mandated to provide health examinations for their workers.
- In Italy, more similarly to the UK, occupational health services are delivered by either certified-occupational physicians or by general physicians who have additional training in occupational medicine.[46] These physicians may be supported by occupational health nurses, health visitors and other professionals.
The UK may learn something about OH service provision from countries with mandatory policies. Although it is not clear which regimes are most effective, there is good evidence that OH services can help employees with health issues stay in work and facilitate their return to work – including for musculoskeletal disorders[47] and common mental disorders (CMDs) such as anxiety and depression.[48] For example, among workers with CMDs, absence can be reduced by consultations with an occupational health psychologist[49] and interventions based on problem-solving.[50]
Moreover, as well as helping workers address health issues head on, OH services can reduce work ill health indirectly. This could be by fostering healthier workplaces and improving lifestyles;[51] or even by increasing workers’ self-efficacy and ability to self-manage, thus reducing anxiety due to working in complex organisations.[52]
However, OH services are by no means guaranteed to be effective. Their impact depends significantly on the type of intervention and the target population.[53],[54] For example, OH services can be more effective when they are tailored and targeted at workers who are at higher risk of sickness absence,[55] or when they are supplemented by a telephone-based service giving earlier access to support.[56]
Sickness absence policies
Paid sickness absence is a common feature of government support within many countries, but there are notable differences in the duration of sickness benefits periods and the amount of sickness pay offered. A report by the Dutch Employee Insurance Agency (UWV) compares eight European countries and highlights that the UK is unusual in that statutory sick pay is not linked to an individual’s wages but is a fixed amount.[57] In other countries, by contrast, the payment is made by the employer based on income earned by the employee before their illness and ranges from 70–100%.
More specific examples include:
- In Finland, provided that a worker’s employment contract has lasted longer than one month, employers are obliged to pay the first 10 days of employees’ sick leave at 100% of the worker’s salary.[58] After this initial 10-day period, employees can collect sick pay for a maximum of 300 days from Finland’s Society Security Agency. Anyone who has not recovered after this time may qualify for a disability pension.
- In Italy, sickness absence is managed by a GP, and subject to verification by local authorities.[59] After 60 days of absence, a medical examination is required and a statement is made on the worker’s ability to undertake temporary or part-time work, as well as a recommended timeframe for a return to work (where applicable) and adjustments that may be required.
The UK may wish to consider these different approaches when supporting employee health and return to work. Research suggests that countries with higher levels of sickness benefits and longer benefit durations tend to see higher rates of sickness absenteeism, as one might expect.[60] However, a study exploring the longer-term impacts of sickness benefits found that higher sickness benefits may have a protective impact on employee health.[61] Our own analysis in Section 2 supports the idea that higher sickness pay is compatible with strong employment outcomes, as seen in some Scandinavian countries with higher levels of sickness pay (see Figures 7 and 8).
Some countries have transferred responsibility for paying sickness benefits from government to employers as a means of reducing rates of sickness absence. Employers have, however, raised concerns regarding medicalisation in the workplace and the difficulties of delineating job-related stress from other contributing factors. Further, the level of support provided to those in precarious work – for example, agency work or zero-hours contracts – varies greatly between systems, with some offering significantly less support to this group.[62]
Return to work
To make the transition back into work following sickness absence, workers benefit from support with rehabilitation and workplace adjustments. While these practices are adopted by some employers in the UK and adjustments for workers with disabilities can be required under the Equality Act 2010, more comprehensive provisions are evident in some other countries.
- Various countries – including Austria, Denmark, Finland, Germany, the Netherlands, Norway and Sweden – emphasise prevention and early intervention, with employers holding broad responsibilities in the return-to-work process. Support typically also includes the effective coordination of multi-disciplinary teams and a case management approach, ensuring holistic support and a structured pathway back to work.[63]
- More specifically, Finland additionally takes a proactive approach to support a partial return to work, offering greater flexibility and in principle enabling more people to return to work. A partial sickness benefit scheme is available to those who qualify for full sick pay. This is available for up to 150 days and supports a part-time return to work for those employees who can perform reduced or modified tasks (that will not pose a risk to their health or recovery) through part-time work.[64]
- In Canada, a Type B country, tools are made available to employers to support them in developing return to work plans for their staff.[65] Employers are required to make adjustments for staff with disabilities, illness or injury. Beyond this, a remain-at-work or return-to-work plan can be created (sometimes with the support of occupational health professionals). However, there is no legislative mandate for employers to provide rehabilitation support for all employees, making this approach more similar to the UK.
It is important that any return to work ensures that employees do not return to poorer quality jobs. This requires a considered and holistic approach to workplace adjustments. Research shows that levels of support for return-to-work initiatives vary greatly between countries, suggesting that government policies and incentives have a significant impact on this area.[66] Those approaches that actively engage with employers, employees and health practitioners are more successful than others and the UK may wish to further understand such approaches.[67],[68]
Getting into work: Supporting engagement or re-engagement for those outside the labour market
Many countries have active labour market policies and public employment services designed to support people with ill health or disabilities into work. As well as requirements for employers to engage in return-to-work planning (see above), these can include schemes to support workplace adjustments, anti-discrimination legislation and financial incentives to employers.[69] People with health limitation and disabilities often face multiple barriers that reduce their employment chances. To be successful, employment programs must provide tailored support to meet individual needs.[70]
Anti-discrimination legislation
Anti-discrimination legislation requires employers to make adjustments for people with disabilities and not be biased against them in recruitment and promotion decisions. They include:
- Human Rights Act/Employment Equity Act 1996 in Canada.
- Act on Prohibition of Discrimination in the labour market 2004 in Denmark.
- Working Environment Act 1977/2005 in Norway.
- Prohibition of Discrimination in Working Life of People with Disability Act 1999 in Sweden.
- Disability Discrimination Act (DDA) 1995 and Equality Act 2010 in the UK.
Evidence on the UK DDA suggests little impact: its introduction did not lead to improvements in employment rates at the population level for people with long-standing illness.[71] Indeed, for some groups – in particular, female and lower skilled disabled workers and those with mental health conditions – employment rates appeared to worsen after the DDA was introduced (however, this does not appear to be as a result of the DDA).
Quotas
In contrast to the UK, where quotas are not legal in normal employment situations, several countries have established positive discrimination frameworks to encourage the employment of disabled people, identifying quotas for their employment.[72] Financial incentives and penalties have also been used to encourage the recruitment of disabled workers (sometimes in addition to mandated quotas). Such countries include France, Germany, Italy and Japan.
- Japanese employers who fail to meet their quota pay a levy, while those who exceed their quota receive an allowance for every person they employ above the required number.[73] Further, the Japanese government provides grants to employers for upgrading the workplace environment, developing the skills of disabled people and hiring job coaches.
- In France, employers with over 20 employees are required to have disabled workers representing 6% of their overall workforce. Financial penalties are in place for those who do not comply.
- In Italy, social cooperatives can be used to help organisations employ workers with disabilities to ensure the effective implementation of quotas. Agreements can be made with Public Employment Services and individual employers can be made to support the integration of people with disabilities (defining the conditions related to the hiring of workers with disabilities, the tasks assigned to them and the specific support and monitoring actions needed).
Research suggests that quota systems can be challenging to implement effectively and may result in unintended negative outcomes, such as disabled people being employed in lower-skilled and lower-paid roles.[74] These outcomes could be the result of how quota systems are designed and implemented, including the level of the quota, rather than the existence of a quota system per se. Data suggests that European quota systems are associated with narrower gaps between the employment of disabled and non-disabled individuals.[75] This may be evidence that the UK would do well to adopt these approaches, but a causal relationship is unclear: it could instead be that certain types of countries are more likely to operate quotas.
Workplace adjustments
As for workers returning from sick leave (see above), workplace adjustments for those transitioning out of long-term economic inactivity should be holistic, carefully considered and not superficial. Workplace adjustments for ill health or disability may include physical changes, such as adapting buildings or providing specialist equipment. They can also involve changes to employment – including reduced hours, flexible working schedules and role modifications – or the provision of support to workers (e.g. a sign language interpreter). Although workplace adjustments are recommended for disabled employees in the UK and schemes like Access to Work can provide financial aid to organisations to make certain adjustments, the examples below highlight different models through which workplace adjustments are provided:
- In Norway, a government-supported system exists such that employers can access advice from specialised professionals in local public employment offices. As well as guidance, this support includes employer compensation for adjustments and wage subsidies for reduced work capacity or productivity.[76]
- In Canada, most costs of workplace adjustments are covered by employers, but this is supplemented by time-limited publicly funded support.[77] Nationally this is enabled through the Labour Market Agreement for People with Disabilities and the Opportunities Fund. At a provincial level, Workers’ Compensations Boards also provide support for workers injured within the workplace.
- In Australia, the Job Access Programme provides employers with a range of tools to support workplace adjustments and modifications for employees with disabilities. Services include access to trained advisors via a telephone service, and online resources including a toolkit and claims process for the payment of workplace modifications.[78]
Evidence suggests that well-designed workplace adjustments can successfully increase the employment rates of people with health limitations. The more effective adjustments tend to address fundamental aspects of job quality – that is to say, the nature of the work and the environment in which it is performed. For example, these could include giving employees greater flexibility in their work schedules or control over work methods, team building or training that strengthens managerial and peer support; it could also relate to having effective channels for employee voice and representation (see section above on healthy work). By focusing on employee’s day-to-day roles, such interventions can enable a preventative approach that helps employees stay in good health on their return to work.
However, workplace adjustments have historically had low uptake and often been less accessible to workers in lower-skilled jobs.[79] To be impactful at a national level, they need to be implemented more widely and consistently.
Financial incentives for employers
In some Type A countries, employers can access wage subsidies to offset the (real or perceived) costs associated with employing or retaining workers with health limitations.
- In Norway, the Active Sick Leave (ASL) programme was introduced to provide a 100% wage subsidy for employees with a reduced work capacity to enable them to return to work.[80] To access this funding employers must comply with certain obligations – e.g. contacting the health care system for an employee rehabilitation assessment after four weeks of sick leave.
- In Denmark, the Flexjobs national programme enables employers of 18- to 59-year-olds with disabilities to claim up to two-thirds of the disabled employee’s wages as a subsidy.[81] This programme can also support reductions in working hours or be used to enable workplace adjustments.
- In the Netherlands, the ‘Trial Placement’ initiative provides employers with wage subsidies for a two-month period, enabling them to hire employees with disabilities on a temporary basis. Measures are in place to prevent misuse, including the requirement that a permanent job opportunity must exist, and employers must declare in advance their intention to hire the candidate for at least six months after the trial period. Results suggest that in about half of cases, the candidate is retained.[82]
Norway’s ASL programme faced challenges with low take up, although efforts to improve participation have shown some success. Evidence on its impact is mixed; the most rigorous study, focused on workers with lower back pain, found no significant impact on outcomes after a year.[83]
A study of Denmark’s Flexjobs programme found that people with reduced work capacity generally did not see improved chances of employment, although benefits were noted for those aged 35-44.[84] Improvements were also observed among disabled people without reduced work capacity, though this group was not the programme’s intended focus. Further research found that subsidised jobs tended to be lower-skilled and lower-paid, with these roles viewed negatively by other employees and society. The programme risked being perceived more as a social obligation than a way to enable people to participate meaningfully in the economy, potentially disempowering workers with disabilities.[85]
Overall, policy makers have various options for creating financial incentives for employers, but the evidence base on whether these actually aid the employment of workers with health limitations is mixed.
4. Discussion and conclusions
This report finds that the UK could do much better in enabling people with long-term illnesses or disabilities to stay in or get back into employment. Recently, problems have been highlighted with the quality of LFS data; in fact this is a common challenge in national statistics across other countries, due to declining response rates. Nonetheless, based on the best current data we have, the UK has among the largest employment gaps between people with and without health limitations compared to its European peers. Various points of data suggest that the UK has scope room for improvement and younger workers should be a priority.
Drawing policy lessons from other countries is not straightforward. Economic and social policies reflect a range of factors – institutional, historic, cultural, social and economic – and what works in one place may not work in another. We thus approach comparisons with some caution and remain open-minded about the application to the UK.
Moreover, evidence on individual initiatives is mixed, with several areas yielding limited or inconsistent results. For example, initiatives like wage subsidies have demonstrated benefits in specific contexts but have also faced challenges, such as low uptake or unintended outcomes. This underlines the need to consider not just individual interventions but the broader factors that shape their success.
Nonetheless, there is clear potential to learn from other contexts and adapt successful policies and practices. There are approaches, such as workplace adjustments and tailored return-to-work programmes, that show clear promise.
In this section we explore some of the key cross-cutting themes that underpin success, drawing on our review of the evidence and insights from our expert workshop.
Potential policy explanations of work-health differences across Europe
The patterns identified in Section 2 of this report may be partly explained by how targeted and tight a country’s policies are. The UK imposes relatively light obligations on employers regarding accommodations for employees with health conditions. Financial assistance is provided through benefits like the Personal Independence Payment (PIP) and Employment and Support Allowance (ESA). However, beyond financial aid, the state’s role in supporting individuals with health conditions in the labour market is minimal.[86]
In contrast, there are tighter regulations on employers in Germany, Denmark, and Spain to integrate employees with health issues. Similarly, Sweden implements tailored support to facilitate return to work with better access to health care.[87]
How structured work-health integration programs are may also play a role. For example, in the Netherlands, the ‘Gatekeeper Improvement Act’ mandates collaboration between employers and employees to facilitate return-to-work processes.[88] In Finland, a tripartite collaboration among government, employers, and trade unions ensures cohesive strategies for workplace inclusion.[89]
Systemic and consistent approaches
A joined-up, system-wide approach to supporting those with ill health or disabilities to work is likely to be key to its effectiveness. This could be a case of effectively linking preventive and rehabilitative measures, or more generally, ensuring that one policy does not undermine another, or ‘covering ones’ bases’ through coordinated policies that tackle different areas through different means.
In this regard, Type A countries with integrated approaches are likely to have the advantage. This is important to note when assessing individual initiatives: even when there is evidence of effectiveness, their impact may be limited if they are implemented in isolation.
A related point is the consistency and longevity of a country’s workplace health policies. Discussion with experts highlighted a contrast between the UK and its neighbours in this regard. While the UK has a relatively strong body of research and has developed well-designed interventions, it was perceived as lacking continuity in its approach to occupational health and workplace wellbeing.
Experts spoken to as part of this report noted that UK policies are often characterised by short-termism, with a focus on new initiatives rather than sustaining and building on existing schemes. Long-term commitment was seen as paramount for achieving sustained improvements in work and health outcomes in the UK. Indeed, it was even argued that it matters less which specific actions the UK government takes, and more that it sticks to a coherent, long-term plan.
We present an example of a more consistent approach as taken in the Netherlands in Box 1 below.
The roles of ‘social partners’ and the market
Countries differ in the extent to which workplace health is shaped by state involvement, employer obligations and market-driven delivery. Proactive government involvement and collaboration with key actors is important for effective work and health systems.
One risk to be aware of in market-led provision is the increasing costs falling on individuals, whether directly or indirectly, leading to gaps in support. While it is not clear that there is one ‘right’ approach, many countries – especially Type A countries – place substantial obligations on employers alongside incentives to encourage desired actions.
| Box 1. The Netherlands: an example of a sustained approach to occupational health policy
When it comes to lifestyle factors, the Netherlands is doing well. The population has relatively low levels of obesity and medium to low levels of both smoking and heavy drinking.[90] In a relatively healthy country, how has policy treated the area of ill health and employment? In the early 1990s, following a period of high levels of labour market inactivity, the Netherlands transferred much of the responsibility for funding sick pay from the state to employers.[91] The Dutch social security system requires employers to pay at least 70% of an employee’s salary for up to two years. Many employers choose to take out insurance to cover sickness absence compensation.[92] Employers are also required to appoint an occupational safety and health service, or an occupational physician, to assist employers who are not able to work due to illness. Further, both employers and employees are required to support reintegration back to work, which may include the provision of reasonable adjustments.[93] Failure to do so can result in benefit cuts for employees and a third year of sick pay to be funded by their employer.[94] There are some notable exceptions. In the case of employees with disabilities, the cost of sick pay is met by the state, acting as an incentive for the employment of disabled people.[95] Similarly, employers are incentivised to provide part-time work opportunities for those fit enough to return to work part-time, as they can also qualify for part-time sick pay funding from the state. It is widely considered that a critical enabler in the Netherlands’ approach has been a pre-existing culture of cooperation between government and social partners and thus active employer involvement. This has arguably dovetailed with another success factor: the Netherlands’ highly competitive OH services market. One can see positive outcomes of the Dutch approach reflected, for example, in 2017 data showing a decline in sickness absence since the early 2000s.[96] Notably, the Netherlands also has relatively low levels of reported stress among full-time employees. However, a fuller picture is more mixed than this would suggest. Our analysis of 2022 data shows that the Netherlands continues to experience relatively high levels of reported health limitations in its working age population and a similar disability/ill-health employment gap to that seen in the UK. Netherlands’ approach has been broadly consistent for several decades. Despite the complexities, research suggests that this is a factor in helping workers to maintain good health and to rehabilitate those who have taken sickness absence.[97],[98] |
Tripartite approaches should help in this regard. More common in some mainland European countries such as Germany and core to the International Labour Organisation, these formally drawing together the ‘social partners’ of government, employers or industry representatives, and employee representatives. Again, models vary significantly, particularly in the degree to which social dialogue is bottom-up, occurring through consultative or democratic mechanisms within individual organisations, or top-down, led by representatives at a national or international level. Such differences likely influence the outcomes of workplace health interventions and policies and shape what approaches are realistic to pursue in the first place. Further research would do well to compare these systems in greater detail.
It is also vital to consider institutional capacity – within public services, social partners, employers, health markets and communities. The extent to which public bodies are proactive has a major influence on the how the ‘social partners’ work together. In addition, employer and government capacity shapes the extent to which there is reliance on private market-led provision. Another important factor is the scale of change that employers can lead or handle themselves.
Two aspects seem pertinent here. First, governments can place fewer demands on the management of workplace health for smaller employers. The Dutch system provides one example, where the same laws apply to all employers, but additional support is provided for small firms. Second, industry-wide schemes offer opportunities for sharing lessons and good practice between organisations. This could be larger firms with greater resources leading the way, but smaller employers can also contribute valuable insights. Both public and private sector employers likely have useful lessons to share. In short, both targeted support for smaller employers and industry-wide knowledge-sharing should help with implementation and outcomes.
Awareness, engagement and attitudes
Having well-designed policies and interventions in place is not in itself sufficient. A crucial next step is to figure out how they can be implemented so that they gain traction in practice.
Most countries struggle to some extent with increasing the uptake of policy interventions on work and health. Raising awareness among key actors of the available support and their responsibilities is an obvious step. This may be easier in Type A countries, where leading agencies can actively raise awareness of available support among the working population (this relates to how the ‘social partners’ work together – see above).
Our discussion with experts suggested that attitudes towards ill health and workplace health policy are also influential. One general aim should be to de-stigmatise physical and mental ill health in the workplace, to reduce under-reporting and increase chances of rehabilitation. In various ways, avoiding the ‘over-medicalisation’ of occupational health services would seem to be helpful. This could include: making OH services more accessible by focusing on broader, non-clinical support; promoting general workforce health as well as treating ill health; and ensuring a clear focus on work capacity alongside health issues. This will be shaped by the mindset and expectations of physicians and others involved in providing OH.
Differences in attitudes towards and the reporting of ill health may complicate the cross-country comparisons but also provide valuable insights. For example the Netherlands and Finland (both Type A countries) have high levels of reported health limitations in their populations alongside high employment of people with health limitations (i.e. narrow ill-health employment gaps). Conversely, the Republic of Ireland (a Type B country, with a less integrated approach to workplace health) has a low level of reported health limitations among its population and a relatively wide disability/ill-health employment gap.
It is difficult to explain such differences with any confidence, but it is fairly likely that part of the reason lies in differences in reporting. There are various ways this could influence our findings. For example, people reporting health limitations may typically be referring to more severe conditions in some countries than others, making the effect of health limitations appear greater. At the same time, a more coordinated approach and better access to support may encourage higher levels of reporting (this could help explain trends in the Netherlands and Finland). On the other hand, there could be a risk that the more proactive approaches to workplace health inadvertently increase workers’ sensitivity to job-related stress, potentially resulting in higher perceived stress levels.[99]
Concluding remarks
This report centres on cross-country comparisons in labour market trends and policy. This is a useful perspective, but as is highlighted in our observations about attitudes and reporting, complexities arise because of the political, economic and social factors of different countries.
Nonetheless, we can make some conclusions with a degree of confidence. Most strikingly, there is a compelling case for the UK to improve employment support for people with ill health and disabilities. Although it is not the worst performer among the 15 European countries we examined, the UK consistently ranks among the worst performing countries on most key measures. Without action, the trends identified in our analysis could have significant long-term consequences for the economy, society, and individuals’ quality of life.
Change needs to happen across the board, but younger workers should be a top priority.
This report highlights a wealth of international examples of policy interventions that differ in strength, mechanism and scope. Careful consideration should now be given to what changes are most likely to lead to sustained improvements in the UK, enabling more people with long-term ill health or disabilities to benefit from employment and actively contribute to the economy.
References
Axén, I., Brämberg, E., Vaez, M., Lundin, A., & Bergström, G. (2020). Interventions for common mental disorders in the occupational health service: a systematic review with a narrative synthesis. International Archives of Occupational and Environmental Health, 93, 823 – 838. https://doi.org/10.1007/s00420-020-01535-4.
Belin A, Dupont C, Oulès L, Kuipers Y and Fries-Tersch E (2016) Rehabilitation and return to work: Analysis report on EU and Member States policies, strategies and programmes. Luxembourg: European Agency for Safety and Health at Work. https://osha.europa.eu/sites/default/files/rehabilitation_and_return_to_work_analysis_summary.pdf.
BIS.(2014) The Impact of the Working Time Regulations on the UK labour market: A review of evidence. Department for Business, Innovation and Skills. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/389676/bis-14-1287-the-impact-of-the-working-time-regulations-on-the-uk-labour-market-a-review-of-evidence.pdf
Braun, T., Bambra, C., Booth, M., Adetayo, K., & Milne, E. (2015). Better health at work? An evaluation of the effects and cost-benefits of a structured workplace health improvement programme in reducing sickness absence. Journal of public health, 37 1, 138-42 . https://doi.org/10.1093/pubmed/fdu043.
Brown, J., Mackay, D., Demou, E., Craig, J., Frank, J., & Macdonald, E. (2015). The EASY (Early Access to Support for You) sickness absence service: a four-year evaluation of the impact on absenteeism. Scandinavian journal of work, environment & health, 41 2, 204-15 . https://doi.org/10.5271/sjweh.3480.
- Carroll, J. Rick, H. Pilgrim, Jackie Cameron, J. Hillage. 2010. Workplace involvement improves return to work rates among employees with back pain on long-term sick leave: a systematic review of the effectiveness and cost-effectiveness of interventions. Disability and Rehabilitation. 10.3109/09638280903186301
Chaupain-Guillot, S., & Guillot, O. (2017). Sickness Benefit Rules and Work Absence: An Empirical Study Based on European Data. Revue D Economie Politique, 127, 1109-1137. https://doi.org/10.3917/REDP.276.1109.
Crane, M., Bohn-Goldbaum, E., Lloyd, B., Rissel, C., Bauman, A., Indig, D., Khanal, S., & Grunseit, A. (2019). Evaluation of Get Healthy at Work, a state-wide workplace health promotion program in Australia. BMC Public Health, 19. https://doi.org/10.1186/s12889-019-6493-y.
Datta Gupta N, Larsen M. Evaluating employment effects of wage subsidies for the Disabled – the Danish Flexjobs Scheme. Annual Conference European Association Labour Economists. 18–20 September, Amsterdam, 2008.
Devine, A., Shields, M., Dimov, S., Dickinson, H., Vaughan, C., Bentley, R., Lamontagne, A., & Kavanagh, A. (2021). Australia’s Disability Employment Services Program: Participant Perspectives on Factors Influencing Access to Work. International Journal of Environmental Research and Public Health, 18. https://doi.org/10.3390/ijerph182111485.
Doellgast, V., & Berg, P. (2018). Negotiating Flexibility: External Contracting and Working Time Control in German and Danish Telecommunications Firms. ILR Review, 71, 117 – 142. https://doi.org/10.1177/0019793917703659.
DWP (2021). International comparison of occupational health systems and provisions. London: Department for Work and Pensions. www.gov.uk/government/publications/international-comparison-of-occupational-health-systems-and-provisions.
DWP. (2019, May 15). Full report: Understanding self-employment for people with disabilities and health conditions. GOV.UK. https://www.gov.uk/government/publications/self-employment-for-people-with-disabilities-and-health-conditions/understanding-self-employment-for-people-with-disabilities-and-health-conditions.
Eurofound (2021). Disability and labour market integration: Policy trends and support in EU Member States, Publications Office of the European Union, Luxembourg. www.eurofound.europa.eu/system/files/2021-04/ef20013en.pdf.
Eurofound (2021). Right to disconnect. Online article. www.eurofound.europa.eu/en/european-industrial-relations-dictionary/right-disconnect
Eurostat (undated) EU statistics on income and living conditions https://ec.europa.eu/eurostat/web/microdata/european-union-statistics-on-income-and-living-conditions.
Grammenos, S. (2013). European comparative data on People with disabilities & Citizenship. 10.13140/RG.2.2.26602.82884.
Hemmings, P. and C. Prinz (2020) Sickness and disability systems: comparing outcomes and policies in Norway with those in Sweden, the Netherlands and Switzerland, OECD Economics Department Working Papers, No. 1601, OECD Publishing, Paris, https://doi.org/10.1787/c768699b-en.
Hohnen P. Processes of marginalisation: an analysis of new forms of exclusion on the Danish labour market, Vol. 11. Copenhagen: The Danish National Institute of Social. Research Working Paper, 2001.
Hulls, P., Richmond, R., Martin, R., Chavez-Ugalde, Y., & Vocht, F. (2021). Workplace interventions that aim to improve employee health and well-being in male-dominated industries: a systematic review. Occupational and Environmental Medicine, 79, 77 – 87. https://doi.org/10.1136/oemed-2020-107314.
IES (2024). October Labour Market Statistics: comment from the Institute for Employment Studies. Online article, 16 Oct. https://www.employment-studies.co.uk/news/october-labour-market-statistics-comment-institute-employment-studies-1.
ISER / University of Essex (undated). Understanding Society: The UK Household Longitudinal Study. www.understandingsociety.ac.uk/.
Jones, P. & Bano, N. (2021). The Right to Disconnect. Cranbourne: Autonomy Research. https://autonomy.work/wp-content/uploads/2021/08/the-right-to-disconnect-AutonomyFINAL.pdf.
Joyce, K., Pabayo, R., Critchley, J., & Bambra, C. (2010). Flexible working conditions and their effects on employee health and wellbeing. The Cochrane database of systematic reviews, 2, CD008009 . https://doi.org/10.1002/14651858.CD008009.pub2.
Kankaanpää, E. (2010). Economic incentives as a policy tool to promote safety and health at work. Scandinavian journal of work, environment & health, 36 4, 319-24.
Kela. (2022). Law amendment extends eligibility for partial sickness allowance. Kela / Kansaneläkelaitos. https://www.kela.fi/news/law-amendment-extends-eligibility-for-partial-sickness-allowance.
Koskela, K., & Sauni, R. (2012, November 22). OSH system at national level – Finland – OSHwiki | European Agency for Safety and Health at Work. Oshwiki.osha.europa.eu. https://oshwiki.osha.europa.eu/en/themes/osh-system-national-level-finland.
Labour market information: France. (2023, September 26). Eures.europa.eu. https://eures.europa.eu/living-and-working/labour-market-information/labour-market-information-france_en.
Lahti, J., Harkko, J., Nordquist, H., Piha, K., Pietiläinen, O., Mänty, M., Rahkonen, O., Lallukka, T., & Kouvonen, A. (2021). Seeing an occupational health psychologist reduces sickness absence due to mental disorders: A quasi-experimental study. Preventive medicine, 106611. https://doi.org/10.1016/j.ypmed.2021.106611.
Lalive, R., Wuellrich, J., Zweimüller, J. (2009). Do Financial Incentives for Firms Promote Employment of Disabled Workers? A Regression Discontinuity Approach. NRN working paper. The Austrian Center for Labor Economics and the Analysis of the Welfare State.
Leoni, T. (2022). Employer support for employees returning to work from sick leave – evidence for Europe. The European Journal of Public Health, 32. https://doi.org/10.1093/eurpub/ckac129.095
Linden, M., Muschalla, B., Hansmeier, T., & Sandner, G. (2014). Reduction of sickness absence by an occupational health care management program focusing on self-efficacy and self-management. Work, 47 4, 485-9 . https://doi.org/10.3233/WOR-131616.
Marsh, G., Lewis, V., Macmillan, J., & Gruszin, S. (2018). Workplace wellness: industry associations are well placed and some are ready to take a more active role in workplace health. BMC Health Services Research, 18. https://doi.org/10.1186/s12913-018-3364-7.
McCann, D. (2005). Working time laws: A global perspective. Findings from the ILO’s Conditions of Work and Employment Database. The International Labor Organization.
Muto, T., Nakahara, T., Woo Nam, E. (2011). Asian Perspectives and Evidence on Health Promotion and Education. 10.1007/978-4-431-53889-9.
Nazarov, Z., Kang, D., & Schrader, S. (2015). Employment Quota System and Labour Market Outcomes of Individuals with Disabilities: Empirical Evidence from South Korea. Fiscal Studies, 36, 99-126. https://doi.org/10.1111/J.1475-5890.2015.12047.X.
NEA. (2023). Working conditions for employees. Netherlands Enterprise Agency.
OECD (2010) Sickness, Disability and Work: Breaking the Barriers A Synthesis of Findings across OECD Countries. Paris: OECD.
OECD (2010). Sickness, Disability and Work breaking the barriers. Paris, OECD. www.oecd.org/content/dam/oecd/en/publications/reports/2010/11/sickness-disability-and-work-breaking-the-barriers_g1g10adb/9789264088856-en.pdf
OECD (2022). Promoting Health and Well-being at Work: Policy and Practices, OECD Health Policy Studies, OECD Publishing, Paris, https://doi.org/10.1787/e179b2a5-en.
Oh, J., & Sol, V. (2008). The policy program improving occupational safety in The Netherlands: An innovative view on occupational safety. Safety Science, 46, 155-163. https://doi.org/10.1016/J.SSCI.2007.05.015.
ONS (2022). Half a million more people are out of the labour force because of long-term sickness. Online article, 10 November. Newport: Office for National Statistics. www.ons.gov.uk/employmentandlabourmarket/peoplenotinwork/economicinactivity/articles/halfamillionmorepeopleareoutofthelabourforcebecauseoflongtermsickness/2022-11-10
ONS (2024). Unemployment rate (aged 16 and over, seasonally adjusted): %. Labour market statistics time series (LMS).
Ose, S. (2022). Precarious work, sickness absence and risk sharing between employers, employees and social insurance. The European Journal of Public Health, 32. https://doi.org/10.1093/eurpub/ckac129.376.
Plomp, H. (2008). The impact of the introduction of market incentives on occupational health services and occupational health professionals: experiences from The Netherlands. Health policy, 88 1, 25-37 . https://doi.org/10.1016/j.healthpol.2008.02.003.
Poll, M., Nybergh, L., Lornudd, C., Hagberg, J., Bodin, L., Kwak, L., Jensen, I., Lohela-Karlsson, M., Torgén, M., & Bergstrom, G. (2020). Preventing sickness absence among employees with common mental disorders or stress-related symptoms at work: a cluster randomised controlled trial of a problem-solving-based intervention conducted by the Occupational Health Services. Occupational and Environmental Medicine, 77, 454 – 461. https://doi.org/10.1136/oemed-2019-106353.
Schaufeli, W., & Kompier, M. (2001). Managing Job Stress in the Netherlands. International Journal of Stress Management, 8, 15-34. https://doi.org/10.1023/A:1009549312628.
Scheel IB, Hagen KB, Herrin J, et al. Blind faith? The effects of promoting active sick leave for back pain patients: a cluster-randomized controlled trial. Spine 2002;27:2734–40.
Sjöberg, O. (2017). Positive welfare state dynamics? Sickness benefits and sickness absence in Europe 1997-2011. Social science & medicine, 177, 158-168 . https://doi.org/10.1016/j.socscimed.2017.01.042
Soentken, M. (2015). Progressive Structural Reforms Proposals for European reforms to reduce inequalities and promote jobs, growth and social investment WATCH INITIATIVE SOCIAL PROGRESS. Ofi cyna Wydawnicza ASPRA-JR, Poland. www.unite.it/UniTE/Engine/RAServeFile.php/f/news/2015_11_30_social_progress_lab_struc_reforms.pdf#page=152
Taimela, S., Justén, S., Aronen, P., Sintonen, H., Läärä, E., Malmivaara, A., Tiekso, J., & Aro, T. (2007). An occupational health intervention programme for workers at high risk for sickness absence. Cost effectiveness analysis based on a randomised controlled trial. Occupational and Environmental Medicine, 65, 242 – 248. https://doi.org/10.1136/oem.2007.033167.
UWV (2023). Insight into work disability systems: An international inventory. Amsterdam: Uitvoeringsinstituut Werknemersverzekeringen (UWV). www.uwv.nl/imagesdxa/insight-into-work-disability-systems-an-international-inventory_tcm94-455170.pdf
Vilsteren, M., Oostrom, S., Vet, H., Franche, R., Boot, C., & Anema, J. (2015). Workplace interventions to prevent work disability in workers on sick leave. The Cochrane database of systematic reviews, 10, CD006955. https://doi.org/10.1002/14651858.CD006955.pub3
Voglino, G., Savatteri, A., Gualano, M., Catozzi, D., Rousset, S., Boietti, E., Bert, F., & Siliquini, R. (2022). How the reduction of working hours could influence health outcomes: a systematic review of published studies. BMJ Open, 12. https://doi.org/10.1136/bmjopen-2021-051131
Wilson, T., Sharma, M. and Gifford, J. (2024) Exploring the interactions between job quality, industries and health. London: The Health Foundation. www.employment-studies.co.uk/resource/exploring-interactions-between-job-quality-industries-and-health
Appendix 1: Research methods
Literature review
This report makes especial use of two existing reports: one published by the UK Department for Work and Pensions[100] and one by the OECD.[101] We built on these with a further review of scientific literature. We used Consensus, a generative AI tool, to aid the literature search and review.[102] We recognise the potential for bias in generative AI tools. Thus, the Consensus app was used mainly to identify relevant studies; to reduce the potential for bias, any generative AI descriptions of studies or summaries of findings were cross-checked against the original material, accessed through Google Scholar or scientific databases such as EBSCO Business Source Elite.
EU-SILC and UKHLS data
The analysis of EU-SILC data provides consistent measures across European Union member states on employment and health, along with a rich variety of other demographic information. We use the EU-SILC data for 2018 and 2022 to examine the association of employment (or the lack of it) and health limitations.
The last year the EU-SILC data included information about the UK was 2018, and 2022 is the most recent year that EU-SILC data was available. While the UK is no longer part of EU-SILC data collection, the UKHLS (aka Understanding Society) collects comparable information for the UK. Hence, we have matched the EU-SILC and UKHLS data to construct a dataset combining information from both sources for 2022. We use 2018 as the basis for gaining insights about health limitations and employment prior to the pandemic, and 2022 as the basis for gaining insights for the post-pandemic period. While there were still occasions of COVID-19 cases being reported in 2022, the bulk of the COVID-19 policies that had been in place to support people during the pandemic had expired by 2022 and/or been discontinued.
We use ‘health limitation’ as the variable of interest, contrasting those who reported having limited or severely limited health (including disabilities), with those who did not report health limitations. An instrument for the EU15 average is also shown across measurements for comparative reasons. We group the same countries for comparability purposes in the 2022 data, but denote these as “EU15*” to acknowledge that the UK was then no longer part of the European Union.
Marginal effects regression analysis
Demographic analysis and correlation statistics provide a partial picture that often does not fully capture the dynamic association between variables of interest. In demographic analysis there is a degree of circularity between prevalence, employment and employment gaps which can make it hard to interpret findings.
Our analysis examined how health limitations affect employment across EU15 countries. We first used a probit regression model, designed to analyse binary outcomes, to predict the effect that having health limitations on the probability of being out of work. The key variable of interest was the presence of health limitations, which we derived from survey responses about having long-term illness or health problems. We also controlled for demographic factors to help improve the accuracy of the analysis and reduce bias.
To understand how this relationship varied by country, we used the interaction between having ill health and country of residence to estimate the effect of ill health on being out of work for each country. Using marginal effects analysis – a statistical technique that isolates the impact of specific variables – we then calculated the value added of the country from the interaction effect. The results show how much living in each country influences the probability of employment for people with health limitations. This approach, applied to datasets from 2018 and 2022, allowed us to quantify the unique effect that each country’s system and circumstances have on employment prospects for people with long-term illness or health problems, while accounting for other factors that might influence employment status.
Appendix 2: Additional figures
Figure A1: Marginal effect that having a health limitation has on the likelihood of being out of work: 25–34-year-olds
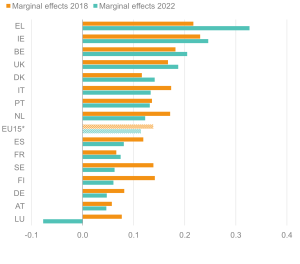
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A2: Marginal effect that having a health limitation has on the likelihood of being out of work: 35–44-year-olds
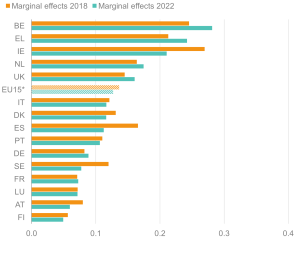
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A3: Marginal effect that having a health limitation has on the likelihood of being out of work: 45–54-year-olds
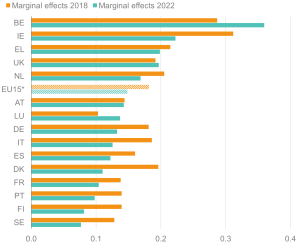
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A4: Marginal effect that having a health limitation has on the likelihood of being out of work: 16–24-year-olds
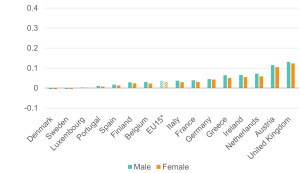
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A5: Marginal effect that having a health limitation has on the likelihood of being out of work: 25–34-year-olds
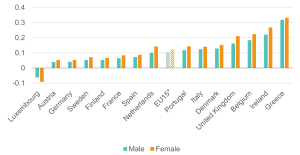
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A6: Marginal effect that having a health limitation has on the likelihood of being out of work: 35–44-year-olds
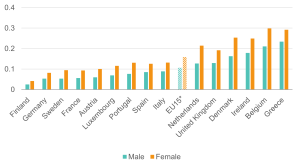
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A7: Marginal effect that having a health limitation has on the likelihood of being out of work: 45–54-year-olds
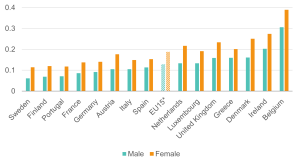
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
Figure A8: Marginal effect that having a health limitation has on the likelihood of being out of work: 55–64-year-olds
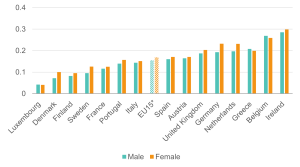
Source: Institute for Employment Studies analysis of EU-SILC and Understanding Society
[1] Comparing statistics between countries is complicated due to a range of factors, such as age differences in the working population, differing definitions of employment status, varying response rates, and varying labour market regulations.
[2] OECD (2010) Sickness, Disability and Work: Breaking the Barriers A Synthesis of Findings across OECD Countries. Paris: OECD.
[3] Eurostat (undated) EU statistics on income and living conditions https://ec.europa.eu/eurostat/web/microdata/european-union-statistics-on-income-and-living-conditions
[4] ISER / University of Essex (undated). Understanding Society: The UK Household Longitudinal Study. www.understandingsociety.ac.uk/
[5] Limitations in cross-country data comparisons can stem from a variety of reasons, such as labour market definitions (e.g. age ranges for working population, definitions of employment status, different ways of counting multiple job-holders), data collection methods (e.g. handling of missing data, varying response rates), statistical treatment (e.g. proxy interviews, sampling techniques, handling outliers, managing seasonality and/or business cycles), and institutional factors (e.g. different unemployment benefit systems, different policy implementation timing, varying labour market regulations). While these factors introduce a level of uncertainty into cross-country comparisons, the data remain a valuable resource for analysis.
[6] IES (2024). October Labour Market Statistics: comment from the Institute for Employment Studies. Online article, 16 October 2024. https://www.employment-studies.co.uk/news/october-labour-market-statistics-comment-institute-employment-studies-1
[7] Resolution Foundation (2024). Get Britain’s Stats Working: Exploring alternatives to Labour Force Survey estimates. https://www.resolutionfoundation.org/publications/get-britains-stats-working/
[8] ONS (2022). Half a million more people are out of the labour force because of long-term sickness. Online article. Newport: Office for National Statistics. www.ons.gov.uk/employmentandlabourmarket/peoplenotinwork/economicinactivity/articles/halfamillionmorepeopleareoutofthelabourforcebecauseoflongtermsickness/2022-11-10
[9] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[10] The EU15* average covers the original EU15 countries post-Brexit, i.e. including the UK.
[11] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[12] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[13] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[14] OECD (2022). Disability, Work and Inclusion: Mainstreaming in All Policies and Practices, OECD Publishing, Paris. https://doi.org/10.1787/1eaa5e9c-en.
[15] DWP (2021). International comparison of occupational health systems and provisions. London: Department for Work and Pensions. www.gov.uk/government/publications/international-comparison-of-occupational-health-systems-and-provisions
[16] Wilson, T., Sharma, M. and Gifford, J. (2024). Exploring the interactions between job quality, industries and health. London: The Health Foundation. www.employment-studies.co.uk/resource/exploring-interactions-between-job-quality-industries-and-health
[17] McCann, D. (2005). Working time laws: A global perspective. Findings from the ILO’s Conditions of Work and Employment Database. The International Labor Organization.
[18] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[19] Doellgast, V., & Berg, P. (2018). Negotiating Flexibility: External Contracting and Working Time Control in German and Danish Telecommunications Firms. ILR Review, 71, 117 – 142. https://doi.org/10.1177/0019793917703659 .
[20] Eurofound (2021). Right to disconnect. Online article. https://www.eurofound.europa.eu/en/european-industrial-relations-dictionary/right-disconnect
[21] Jones, P. & Bano, N. (2021). The Right to Disconnect. Cranbourne: Autonomy Research. https://autonomy.work/wp-content/uploads/2021/08/the-right-to-disconnect-AutonomyFINAL.pdf
[22] Voglino, G., Savatteri, A., Gualano, M., Catozzi, D., Rousset, S., Boietti, E., Bert, F., & Siliquini, R. (2022). How the reduction of working hours could influence health outcomes: a systematic review of published studies. BMJ Open, 12. https://doi.org/10.1136/bmjopen-2021-051131.
[23] Joyce, K., Pabayo, R., Critchley, J., & Bambra, C. (2010). Flexible working conditions and their effects on employee health and wellbeing. The Cochrane database of systematic reviews, 2, CD008009 . https://doi.org/10.1002/14651858.CD008009.pub2.
[24] BIS.(2014) The Impact of the Working Time Regulations on the UK labour market: A review of evidence. Department for Business, Innovation and Skills.
[25] Wilson, T., Sharma, M. and Gifford, J. (2024). Exploring the interactions between job quality, industries and health. London: The Health Foundation. www.employment-studies.co.uk/resource/exploring-interactions-between-job-quality-industries-and-health
[26] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[27] OECD. (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[28] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[29] NEA. (2023). Working conditions for employees. Netherlands Enterprise Agency.
[30] Doellgast, V., & Berg, P. (2018). Negotiating Flexibility: External Contracting and Working Time Control in German and Danish Telecommunications Firms. ILR Review, 71, 117 – 142. https://doi.org/10.1177/0019793917703659.
[31] Doellgast, V., & Berg, P. (2018). Negotiating Flexibility: External Contracting and Working Time Control in German and Danish Telecommunications Firms. ILR Review, 71, 117 – 142. https://doi.org/10.1177/0019793917703659.
[32] Kankaanpää, E. (2010). Economic incentives as a policy tool to promote safety and health at work. Scandinavian journal of work, environment & health, 36 4, 319-24.
[33] Plomp, H. (2008). The impact of the introduction of market incentives on occupational health services and occupational health professionals: experiences from The Netherlands. Health policy, 88 1, 25-37 . https://doi.org/10.1016/j.healthpol.2008.02.003.
[34] OECD. (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[35] OECD. (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[36] Crane, M., Bohn-Goldbaum, E., Lloyd, B., Rissel, C., Bauman, A., Indig, D., Khanal, S., & Grunseit, A. (2019). Evaluation of Get Healthy at Work, a state-wide workplace health promotion program in Australia. BMC Public Health, 19. https://doi.org/10.1186/s12889-019-6493-y.
[37] Plomp, H. (2008). The impact of the introduction of market incentives on occupational health services and occupational health professionals: experiences from The Netherlands. Health policy, 88 1, 25-37 . https://doi.org/10.1016/j.healthpol.2008.02.003.
[38] Wilson, T., Sharma, M. and Gifford, J. (2024) Exploring the interactions between job quality, industries and health. London: The Health Foundation. www.employment-studies.co.uk/resource/exploring-interactions-between-job-quality-industries-and-health
[39] OECD. (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[40] OECD. (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.
[41] Oh, J., & Sol, V. (2008). The policy program improving occupational safety in The Netherlands: An innovative view on occupational safety. Safety Science, 46, 155-163. https://doi.org/10.1016/J.SSCI.2007.05.015.
[42] Hulls, P., Richmond, R., Martin, R., Chavez-Ugalde, Y., & Vocht, F. (2021). Workplace interventions that aim to improve employee health and well-being in male-dominated industries: a systematic review. Occupational and Environmental Medicine, 79, 77 – 87. https://doi.org/10.1136/oemed-2020-107314.
[43] Marsh, G., Lewis, V., Macmillan, J., & Gruszin, S. (2018). Workplace wellness: industry associations are well placed and some are ready to take a more active role in workplace health. BMC Health Services Research, 18. https://doi.org/10.1186/s12913-018-3364-7.
[44] DWP (2021). International comparison of occupational health systems and provisions. London: Department for Work and Pensions.
[45] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions
[46] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions
[47] Vilsteren, M., Oostrom, S., Vet, H., Franche, R., Boot, C., & Anema, J. (2015). Workplace interventions to prevent work disability in workers on sick leave. The Cochrane database of systematic reviews, 10, CD006955. https://doi.org/10.1002/14651858.CD006955.pub3.
[48] Axén, I., Brämberg, E., Vaez, M., Lundin, A., & Bergström, G. (2020). Interventions for common mental disorders in the occupational health service: a systematic review with a narrative synthesis. International Archives of Occupational and Environmental Health, 93, 823 – 838. https://doi.org/10.1007/s00420-020-01535-4.
[49] Lahti, J., Harkko, J., Nordquist, H., Piha, K., Pietiläinen, O., Mänty, M., Rahkonen, O., Lallukka, T., & Kouvonen, A. (2021). Seeing an occupational health psychologist reduces sickness absence due to mental disorders: A quasi-experimental study. Preventive medicine, 106611. https://doi.org/10.1016/j.ypmed.2021.106611.
[50] Poll, M., Nybergh, L., Lornudd, C., Hagberg, J., Bodin, L., Kwak, L., Jensen, I., Lohela-Karlsson, M., Torgén, M., & Bergstrom, G. (2020). Preventing sickness absence among employees with common mental disorders or stress-related symptoms at work: a cluster randomised controlled trial of a problem-solving-based intervention conducted by the Occupational Health Services. Occupational and Environmental Medicine, 77, 454 – 461. https://doi.org/10.1136/oemed-2019-106353.
[51] Braun, T., Bambra, C., Booth, M., Adetayo, K., & Milne, E. (2015). Better health at work? An evaluation of the effects and cost-benefits of a structured workplace health improvement programme in reducing sickness absence. Journal of public health, 37 1, 138-42 . https://doi.org/10.1093/pubmed/fdu043.
[52] Linden, M., Muschalla, B., Hansmeier, T., & Sandner, G. (2014). Reduction of sickness absence by an occupational health care management program focusing on self-efficacy and self-management. Work, 47 4, 485-9 . https://doi.org/10.3233/WOR-131616.
[53] Vilsteren, M., Oostrom, S., Vet, H., Franche, R., Boot, C., & Anema, J. (2015). Workplace interventions to prevent work disability in workers on sick leave. The Cochrane database of systematic reviews, 10, CD006955 . https://doi.org/10.1002/14651858.CD006955.pub3.
[54] Vilsteren et al 2015 (ibid)
[55] Taimela, S., Justén, S., Aronen, P., Sintonen, H., Läärä, E., Malmivaara, A., Tiekso, J., & Aro, T. (2007). An occupational health intervention programme for workers at high risk for sickness absence. Cost effectiveness analysis based on a randomised controlled trial. Occupational and Environmental Medicine, 65, 242 – 248. https://doi.org/10.1136/oem.2007.033167.
[56] Brown, J., Mackay, D., Demou, E., Craig, J., Frank, J., & Macdonald, E. (2015). The EASY (Early Access to Support for You) sickness absence service: a four-year evaluation of the impact on absenteeism. Scandinavian journal of work, environment & health, 41 2, 204-15 . https://doi.org/10.5271/sjweh.3480.
[57] UWV (2023). Insight into work disability systems: An international inventory. Amsterdam: Uitvoeringsinstituut Werknemersverzekeringen (UWV). www.uwv.nl/imagesdxa/insight-into-work-disability-systems-an-international-inventory_tcm94-455170.pdf
[58] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[59] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[60] Chaupain-Guillot, S., & Guillot, O. (2017). Sickness Benefit Rules and Work Absence: An Empirical Study Based on European Data. Revue D Economie Politique, 127, 1109-1137. https://doi.org/10.3917/REDP.276.1109.
[61] Sjöberg, O. (2017). Positive welfare state dynamics? Sickness benefits and sickness absence in Europe 1997-2011. Social science & medicine, 177, 158-168 . https://doi.org/10.1016/j.socscimed.2017.01.042.
[62] Ose, S. (2022). Precarious work, sickness absence and risk sharing between employers, employees and social insurance. The European Journal of Public Health, 32. https://doi.org/10.1093/eurpub/ckac129.376.
[63] Belin A, Dupont C, Oulès L, Kuipers Y and Fries-Tersch E (2016) Rehabilitation and return to work: Analysis report on EU and Member States policies, strategies and programmes. Luxembourg: European Agency for Safety and Health at Work. https://osha.europa.eu/sites/default/files/rehabilitation_and_return_to_work_analysis_summary.pdf
[64] Kela. (2022). Law amendment extends eligibility for partial sickness allowance. Kela / Kansaneläkelaitos. https://www.kela.fi/news/law-amendment-extends-eligibility-for-partial-sickness-allowance.
[65] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions
[66] Leoni, T. (2022). Employer support for employees returning to work from sick leave – evidence for Europe. The European Journal of Public Health, 32. https://doi.org/10.1093/eurpub/ckac129.095.
[67] C. Carroll, J. Rick, H. Pilgrim, Jackie Cameron, J. Hillage. 2010. Workplace involvement improves return to work rates among employees with back pain on long-term sick leave: a systematic review of the effectiveness and cost-effectiveness of interventions. Disability and Rehabilitation. 10.3109/09638280903186301
[68] Clayton, S., Barr, B., Nylén, L., Burström, B., Thielen, K., Diderichsen, F., Dahl, E., & Whitehead, M. (2012). Effectiveness of return-to-work interventions for disabled people: a systematic review of government initiatives focused on changing the behaviour of employers. European journal of public health, 22 3, 434-9 . https://doi.org/10.1093/eurpub/ckr101.
[70] Devine, A., Shields, M., Dimov, S., Dickinson, H., Vaughan, C., Bentley, R., Lamontagne, A., & Kavanagh, A. (2021). Australia’s Disability Employment Services Program: Participant Perspectives on Factors Influencing Access to Work. International Journal of Environmental Research and Public Health, 18. https://doi.org/10.3390/ijerph182111485.
[72] Lalive, R., Wuellrich, J., Zweimüller, J. (2009). Do Financial Incentives for Firms Promote Employment of Disabled Workers? A Regression Discontinuity Approach. NRN working paper. The Austrian Center for Labor Economics and the Analysis of the Welfare State.
[73] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions
[74] Nazarov, Z., Kang, D., & Schrader, S. (2015). Employment Quota System and Labour Market Outcomes of Individuals with Disabilities: Empirical Evidence from South Korea. Fiscal Studies, 36, 99-126. https://doi.org/10.1111/J.1475-5890.2015.12047.X.
[75] Grammenos, S. (2013). European comparative data on People with disabilities & Citizenship. 10.13140/RG.2.2.26602.82884.
[76] OECD (2010). Sickness, Disability and Work breaking the barriers. Paris, OECD. www.oecd.org/content/dam/oecd/en/publications/reports/2010/11/sickness-disability-and-work-breaking-the-barriers_g1g10adb/9789264088856-en.pdf
[77] Clayton, S., Barr, B., Nylén, L., Burström, B., Thielen, K., Diderichsen, F., Dahl, E., & Whitehead, M. (2012). Effectiveness of return-to-work interventions for disabled people: a systematic review of government initiatives focused on changing the behaviour of employers. European journal of public health, 22 3, 434-9 . https://doi.org/10.1093/eurpub/ckr101
[78] OECD (2010) – ibid.
[79] Clayton, S., Barr, B., Nylén, L., Burström, B., Thielen, K., Diderichsen, F., Dahl, E., & Whitehead, M. (2012). Effectiveness of return-to-work interventions for disabled people: a systematic review of government initiatives focused on changing the behaviour of employers. European journal of public health, 22 3, 434-9 . https://doi.org/10.1093/eurpub/ckr101.
[82] Eurofound (2021). Disability and labour market integration: Policy trends and support in EU Member States, Publications Office of the European Union, Luxembourg. www.eurofound.europa.eu/system/files/2021-04/ef20013en.pdf
[83] Scheel IB, Hagen KB, Herrin J, et al. (2002). Blind faith? The effects of promoting active sick leave for back pain patients: a cluster-randomized controlled trial. Spine; 27:2734–40.
[84] Datta Gupta N, Larsen M. Evaluating employment effects of wage subsidies for the Disabled – the Danish Flexjobs Scheme. Annual Conference European Association Labour Economists. 18–20 September, Amsterdam, 2008.
[85] Hohnen P. Processes of marginalisation: an analysis of new forms of exclusion on the
Danish labour market, Vol. 11. Copenhagen: The Danish National Institute of Social
Research Working Paper, 2001.
[86] DWP. (2019, May 15). Full report: Understanding self-employment for people with disabilities and health conditions. GOV.UK. https://www.gov.uk/government/publications/self-employment-for-people-with-disabilities-and-health-conditions/understanding-self-employment-for-people-with-disabilities-and-health-conditions
[87] Koskela, K., & Sauni, R. (2012, November 22). OSH system at national level – Finland – OSHwiki | European Agency for Safety and Health at Work. Oshwiki.osha.europa.eu. https://oshwiki.osha.europa.eu/en/themes/osh-system-national-level-finland
[88] Soentken, M. (2015). Progressive Structural Reforms Proposals for European reforms to reduce inequalities and promote jobs, growth and social investment WATCH INITIATIVE SOCIAL PROGRESS. Ofi cyna Wydawnicza ASPRA-JR, Poland. https://www.unite.it/UniTE/Engine/RAServeFile.php/f/news/2015_11_30_social_progress_lab_struc_reforms.pdf#page=152
[89] Koskela, K., & Sauni, R. (ibid.)
[90] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices, OECD Health Policy Studies, OECD Publishing, Paris, https://doi.org/10.1787/e179b2a5-en.
[91] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[92] Hemmings, P. and C. Prinz (2020). Sickness and disability systems: comparing outcomes and policies in Norway with those in Sweden, the Netherlands and Switzerland, OECD Economics Department Working Papers, No. 1601, OECD Publishing, Paris, https://doi.org/10.1787/c768699b-en.
[93] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[94] Hemmings, P. and C. Prinz (2020). Sickness and disability systems: comparing outcomes and policies in Norway with those in Sweden, the Netherlands and Switzerland, OECD Economics Department Working Papers, No. 1601, OECD Publishing, Paris, https://doi.org/10.1787/c768699b-en.
[95] DWP. (2021). International Comparison of Occupational Health Systems and Provisions: A Comparative Case Study Review. Department for Work and Pensions.
[96] Hemmings, P. and C. Prinz (2020) Sickness and disability systems: comparing outcomes and policies in Norway with those in Sweden, the Netherlands and Switzerland, OECD Economics Department Working Papers, No. 1601, OECD Publishing, Paris, https://doi.org/10.1787/c768699b-en.
[97] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices, OECD Health Policy Studies, OECD Publishing, Paris, https://doi.org/10.1787/e179b2a5-en.
[98] Hemmings, P. and C. Prinz (2020). Sickness and disability systems: comparing outcomes and policies in Norway with those in Sweden, the Netherlands and Switzerland, OECD Economics Department Working Papers, No. 1601, OECD Publishing, Paris, https://doi.org/10.1787/c768699b-en.
[99] Schaufeli, W., & Kompier, M. (2001). Managing Job Stress in the Netherlands. International Journal of Stress Management, 8, 15-34. https://doi.org/10.1023/A:1009549312628.
[100] DWP (2021). International comparison of occupational health systems and provisions. London: Department for Work and Pensions. www.gov.uk/government/publications/international-comparison-of-occupational-health-systems-and-provisions
[101] OECD (2022). Promoting Health and Well-being at Work: Policy and Practices. OECD Health Policy Studies. The Organization for Economic Cooperation and Development.